

Introduction
Diabetes mellitus (DM) is a rapidly growing chronic metabolic disease. DM onset and progression are related to hyperglycemia, microvascular and macrovascular complications caused by insulin secretion defect and/or its biological function disorder [1]. DM is divided into 3 main groups: DM type 1, type 2, and gestational DM [2]. Type 1 DM is caused by an autoimmune condition attacking the patient’s own insulin-producing beta cells, type 2 DM develops from gradual insulin insensitivity and a decrease in insulin production [1]. Gestational DM is only diagnosed in pregnant women and shares similar pathophysiology with type 2 DM [2]. A significant growth of DM incidence is being observed. According to a prevalence study in 2019 there were approximately 463 million DM patients globally and this figure was expected to increase to 700 million patients in the following 25 years [3].
Long term progression of the disease affects critical organs’ functions. Diabetic retinopathy (DR) is one of the common complications of diabetes. Hyperglycemia can damage the blood-retinal barrier and cause leakage of blood from the central retinal artery, ciliary vessels, and the deep layers of the retina, which triggers ischemic changes in the surrounding retina [4]. The local retinal ischemia causes proliferation of new vessels, which can lead to tractional retinal detachment and resultant vision loss. With successful general diabetic treatment vision acuity can be maintained at an acceptable level. However, according to Semeraro et al. blindness will inevitably occur in about 10% of DR patients [5].
Diabetic retinopathy is divided into non-proliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR). Currently two categories are classified into six stages. Nonproliferative diabetic retinopathy (NPDR) includes stage I: microangioma and small bleeding points, stage II: hard exudates, and stage III: cotton wool spots. Proliferative diabetic retinopathy (PDR) includes stage IV: neovascularization, vitreous hemorrhage, stage V: fibrovascular proliferation, vitreous organization, and stage VI: retinal detachment and resultant blindness caused by stretching [4]. Patients with NPDR are usually asymptomatic and they do not complain about any vision problems. However, when visual impairment occurs, the effectiveness of NPDR treatment is poor [6]. In comparison to NPDR, PDR can cause severe vision loss and lead to complete blindness. Prevalence of DR inevitably corresponds to DM duration. Some research proved that NPDR was present in 25% of patients in 5 years after DM diagnosis, in 60% at 10 years and 80% at 15 years [7]. On the other hand, PDR was found in 2% of patients with DM duration of less than 5 years and in 15.5% of patients who had DM for 15 years or more [8].
Traditional therapies for diabetic retinopathy
Traditional DR therapies include laser therapy, vitrectomy and drugs including anti- vascular endothelial growth factor (VEGF) components and steroids. Supplementary treatment involves controlling glucose, lipid blood levels and hypertension treatment.
Anti-VEGF intravitreal injections are useful in visual acuity improvement in patients with diabetic macular edema (DME). Moreover, the injections are proved to be as effective as panretinal photocoagulation at controlling the complications of PDR, with fewer side effects [9]. Aflibercept, bevacizumab and ranibizumab are the three main types of anti-VEGF agents, but only aflibercept and ranibizumab are authorized for use in DME treatment [10]. Recently new drugs such as brolucizumab, faricimab, and conbercept are being tested in clinical trials as potential next-generation anti-VEGF treatment for DME [11].
DR treatment involves intravitreal injections of steroids – triamcinolone acetonide, fluocinolone acetonide, dexamethasone sodium phosphate – by using their anti-inflammatory effects. According to DRCR Protocol I, the effect of intravitreal triamcinolone and laser was equivalent to that of ranibizumab (RBZ) and laser in a 24-week observation study; however, triamcinolone’s effect started to decline because of cataract formation [12]. The study investigating fluocinolone inserts proved better effectiveness of the drug in patients with chronic DME than in non-chronic DME [13]. This may indicate that chronic DME is chemokine driven whereas non-chronic DME is VEGF driven. It suggests that anti-VEGF drugs may be a better treatment option for non-chronic DME and steroids should be used in chronic DME.
As was previously stated, intravitreal inserts of steroids lead to visual improvement in DME and PDR; however, they are a second-line treatment because of their side effects – intraocular pressure rises and cataract formation.
Laser therapy is applied mainly in patients with proliferative eye fundus changes. Multiple studies emphasize the importance of laser therapy in risk reduction of visual loss. According to Jiang et al., panretinal photocoagulation (PRP) can inhibit neovascularization, improve macular edema and vision, and prevent deterioration of the disease [14]. However, laser therapy has limitations and potential complications such as vitreous hemorrhages and retinal cell destruction. Post-PRP destruction of retinal cells may result in permanent scotomas in the visual field, worse night vision and slow light-to-dark adaptation [15, 16].
Vitrectomy is a possible therapeutic choice in DR cases with retinal neovascularization and intravitreal hemorrhages. Multiple studies have assessed the efficiency of vitrectomy in prevention of visual loss. Nathan et al. proved that early vitrectomy performed in type 1 diabetes resulted in visual acuity of 10/20 or more in 36% of eyes, whereas in 12% of eyes with no attempt of vitrectomy the visual acuity remained the same [17]. According to Brănişteanu et al. there is no significant difference in efficacy of retinal repair between the less invasive technique of 23G vitrectomy and 20G vitrectomy [18].
As glycemia is the major risk factor for developing retinopathy, control of blood glucose seems to be important in DR treatment and prevention. A study by Chew et al. revealed that glycemic control reduced the risk for DR progression by 33% [19]. However, it was proved that a positive effect of low blood glucose levels was observed mainly in early stages of DR, as moderately severe nonproliferative diabetic retinopathy has been defined as the level beyond which no further effect of intensified insulin therapy achieves any benefit over a 6-year period in type 1 diabetes [20].
Hypertension is a well-known risk factor for several chronic conditions such as DM. There have been several studies investigating a potential beneficial role of hypertension treatment in DR prevention. Estacio et al. [21] and Schrier et al. [22] revealed no difference between intensive and moderate blood pressure (BP) control with DR progression in diabetic patients. However, Do et al. in 2015 proved a benefit of more intensive blood pressure control intervention with respect to 4- to 5-year incidence of diabetic retinopathy [23]. Further studies conducted in 2020 suggested that tighter control of BP in participants with both hypertension and diabetes may be helpful in DR prevention [24].
Dyslipidemia is another potential modifiable risk factor of DR progression. Nielsen et al. proved that DM patients with statin therapy had 40% lower risk of DR development in comparison with DM patients with no dyslipidemia treatment [25], whereas other observational studies found no benefit of statins on diabetic retinopathy incidence [26]. However, some studies emphasize a role of another lipid-lowering agent, fenofibrate, in DR development and progression. Although the mechanisms of the positive fenofibrate effect are not entirely clear, FIELD and ACCORD trials proved that the drug delays DR progression [27].
Alternative drug therapies
Alternative drug therapy in DR consists of agents such as pancreatic kininogenase, antioxidants (calcium dobesilate (CaD), N-acetylcysteine (NAC), curcumin, resveratrol) or squalamine. According to the study by Lin et al. pancreatic kininogenase proved to be effective in NPDR treatment by improving microcirculation, anticoagulative and thrombolytic effects [28].
Calcium dobesilate with its antioxidant, antiapoptotic potential is an angioprotective agent that can be used to halt neovascularization and prevent DR progression. Anti- VEGF agents are a commonly used therapeutic option in DR treatment. Intravitreal injections of anti-VEGF by inhibiting vascular proliferation improve PDR patients’ visual acuity and stop progression of the disease.
N-acetylcysteine is an antioxidant scavenging reactive oxygen species (ROS). Moreover, NAC inhibits the inflammatory process and angiogenesis by decreasing expression of pro-inflammatory and pro-angiogenic molecules – ICAM-1 and interleukin (IL)-8 – in activated endothelial and epithelial cells [29]. As diabetic retinopathy pathogenesis relies on both oxidative stress and angiogenesis, NAC revealed satisfactory effects in prevention of DR progression and became an alternative supplement of DR therapy [30].
Curcumin is a natural antioxidant affecting free radicals in multiple mechanisms. It inhibits angiogenesis by decreasing levels of vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF) and increasing the levels of the anti-oxidant enzymes superoxide dismutase (SOD) and catalase [31]. By normalizing diabetic microvasculature- reducing vessel tortuosity, shrinkage and micro-aneurysms creation curcumin is a supplementary therapeutic agent in DR treatment [31].
Resveratrol is a natural polyphenol and antioxidant that can be found in the skin of red grapes and red wine. Braokenhielm et al. [32] demonstrated the inhibition of neovascularization after orally administered treatment of resveratrol. It protects retinal epithelium cells from induced cell death; moreover it can reverse the apoptosis and oxidant production generated by benzo(e)pyrene, a toxic component of cigarette smoke [32]. Both antiangiogenic and antiapoptotic effects of resveratrol are used in cardiovascular diseases and diabetic retinopathy treatment.
Topically used squalamine – an inhibitor of multiple growth factors such as PDGF (platelet-derived growth factor) and b-FGF (basic fibroblast growth factor) – was proved to enhance post-anti-VEGF visual improvement in DR patients; squalamine efficacy in diabetic macular edema (DME) treatment is being assessed in clinical trials [33].
Emerging therapies
Gene therapy
Gene therapy is based on the expression of a specific transgene in order to minimize or cure a medical condition with minimal possible side effects. Gene augmentation, gene-specific targeting and genome editing are commonly used methods of gene therapy [34].
In comparison to other organs, the eye is immune-privileged, so only a few inflammatory events are associated with the introduction of viral particles [35]. Moreover, the eye is a relatively small compartment, so it needs only low doses of a vector for gene delivery [35]. These factors enabled gene-specific targeting to become an alternative option in DR treatment.
There are two groups of genes that have been studied as potential objects for DR gene therapy – targeting retinal vasculopathy and targeting retinal protection.
Selecting the first group of genes aimed to decrease neovascularization and promote angiogenesis by interfering in the intraocular VEGF pathway. Flt23k is an anti-VEGF intraceptor that can interfere with the VEGF pathway and reduce VEGF secretion intracellularly [36]. There have been multiple studies based on animal models examining the efficacy of Flt23k injections in DR progression. Zhang et al. in 2015 proved that adeno-associated virus (AAV)-mediated injections of Flt23k inhibit murine choroidal neovascularization [37]. Several studies proved that AAV2 is the preferable vehicle as it is the focus in the regulation of VEGF signaling [35].
Gene therapy decreasing neovascularization involves microribonucleic acids (RNAs) (miRs). MiRs associated with VEGF were studied as a potential drug preventing PDR. Yang et al. found that miR-15b regulates the expression of VEGF by targeting the 3'-untranslated regions to inhibit their transcription [38]. The study proved that miR-15b expression has an influence on angiogenesis; however, Yang et al. used rats as a PDR animal model and further human based research is required.
Another way of targeting retinal vasculopathy is to use agents with antiangiogenic potential. AAV-mediated injections of pigment epithelium-derived factor (PEDF) succeeded in VEGF level decrease and DR progression [37]. Transduction of AAV-mediated endogenous agents such as angiotensin, endostatin, tissue inhibitor metalloproteinase-3 and calreticulin antiangiogenic domain (CAD) was found to inhibit retinal neovascularization in animal model-based research [12]. DR gene therapy includes inhibitors of cell proliferation such as amino-terminal fragment (ATF) and kringle 1 domain of hepatocyte growth (HGFK1); retinal transduction of the following molecules was found to reduce retinal neovascularization in mice models [39, 40] (Fig. 1).

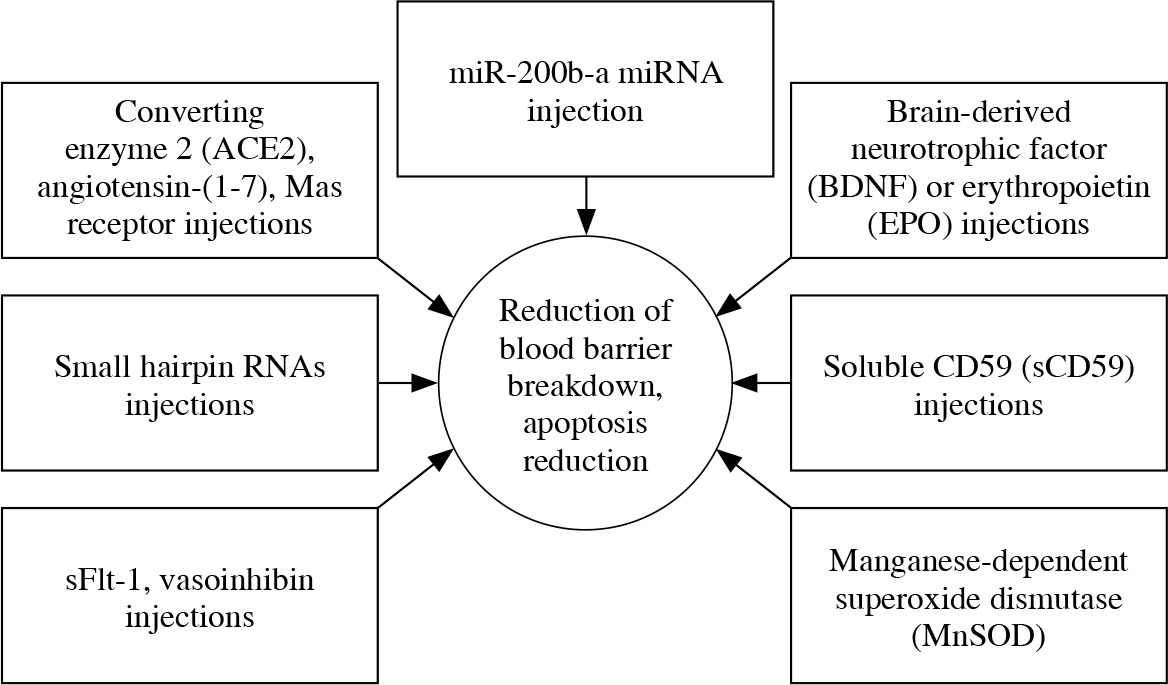
AAV-mediated vectors inhibiting vasopermeability such as sFlt-1 and vasoinhibin were reported as potential DR gene treatments. Injections of these molecules resulted in reduction of blood-retinal barrier breakdown and enhanced some of the retinal functions [41, 42].
The second group of genes that became a target for DR comprises the genes responsible for retinal protection. The treatment is based on affecting oxidative stress and apoptosis reduction and its indications are limited to initial stages of DR.
A significant increase of early growth response 1 (EGR1) expression in vascular cells has been observed in patients with high blood glucose levels. Ao et al. based on this observation used an AAV vector encoding small hairpin RNAs (a molecule silencing gene expression) directed against EGR1 which succeeded in retinal cell apoptosis reduction [43].
Hyperglycemia in diabetes suppresses autophagic activity in diabetes. Mao et al. arrested DR progression in rat models by enhancing the expression of microtubule-associated protein 1 light chain 3-II, a molecule responsible for autophagic activity detection [44].
There were successful trials based on using inhibitors of membrane attack complex to protect retinal neurons from apoptosis. A soluble CD59 (sCD59) – an inhibitor of membrane attack complex – reduced blood-retinal barrier breakdown and vascular leakage by 60% compared with the control group in a mouse model study by Adhi et al. [45]. Furthermore, soluble CD59 was proved to activate retinal glial cells, which are responsible for retinal ganglion cells’ (RGCs) protection from apoptotic stimuli [45].
DR gene therapy targeting retinal protection uses injections of neurotrophic factors. Intravitreal admission of brain-derived neurotrophic factor (BDNF) or erythropoietin (EPO) may induce positive neuroprotective effect by preventing blood-retinal barrier disruption and neuronal apoptosis [25]. Manganese-dependent superoxide dismutase (MnSOD) delivery was also investigated as a potential way of DR gene therapy by decreasing oxidative stress [35].
The development of DR involves oxidative stress-related signaling pathways. MiR-200b, a miRNA, may regulate oxidative stress-related factor oxidation resistance 1 (Oxr1). Yu et al. in their research found that small nucleolar RNA host gene 4 (SNHG4) interacts with miR-200b and inhibits cell apoptosis in DR by upregulating Oxr1 [46].
The renin-angiotensin system (RAS) has been widely studied as a potential pathway for DR treatment. It was proved that RAS inhibitors may be useful in diabetic patients; however, RAS inhibitors currently in use cannot completely prevent the RAS neurodegenerative effect because of the presence of local angiotensin II [29]. Intravitreal injections of AAV-mediated angiotensin-converting enzyme 2 (ACE2), angiotensin-(1-7) and the Mas receptor decreased vascular leakage, inflammation and oxidative stress in diabetes-induced rodents [47] (Fig. 2).
Current studies are finding each year new possible pathways for gene therapy. However, there are multiple limitations of the treatment such as complexity of pathogenesis, safety of the vector delivery of the transgenes, and patient selection due to disease progression.
Mesenchymal stem cells
New DR therapy studies are focusing on the possible regenerative potential of retinal pigment epithelium (RPE). Many ocular diseases such as corneal limbal stem cell deficiency, age-related macular degeneration (AMD), glaucoma, and retinal dystrophies have been proved to be a target of stem cell therapies [48].
According to Gaddam et al. endothelial progenitor cell, embryonic stem cell and mesenchymal stem cell treatment could be a viable option as a prevention of retinal neovascularization and promotion of retinal regeneration in DR [49]. Mesenchymal stem cells (MSC) are found in a variety of different tissues and they have multi-differentiative potential. Due to the simple procedure of isolation and propagation mesenchymal cells derived from bone marrow (BMSCs) are the most commonly used MSCs [50]. BMSCs’ repair potential is based on the ability to express basic fibroblast growth factor (bFGF) and ciliary neurotrophic factor (CNTF).
According to the Huang et al. study endothelial progenitor cells, mesenchymal stem cells and hematopoietic stem cells induce endothelial cell damage repair and halt new pathological retinal vessel formation [50]. The authors did not include adult stem cells and induced pluripotent stem cells in their investigation process, which could be verified in further trials in the future.
In the Huang et al. research streptozotocin (STZ)-induced rats were intravitreally injected with BMSCs and CNTF, to study whether the combination of two agents can enhance the viability of transplanted BMSCs [50]. The research emphasizes the dominant role of CNTF by comparison of BMSC differentiative potential with or without inductive factors pretreatment. Previously CNTF was proved to prolong the perseverance of RPE cells by JAK/STAT3 signaling pathway activation. Huang et al. revealed that CNTF admission alone could influence retinal regeneration by inducing the expression of rhodopsin – both on post-injection days 14 and 21 [50]. The study revealed that CNTF supplement can promote BMSCs’ cytokine secretion and therefore accelerate RPE cell regeneration [50]. Moreover, it was proved that CNTF promote BMSCs’ differentiation into RPE cells – crucial cells in retinal damage repair. The research did not study whether multiple injections could enhance the possible treatment effect, or whether there is a correlation between concentration of CNTF and the final effect. These missing aspects merit further investigation in the future.
SGLT2 inhibitors
Sodium-dependent glucose transporter 2 (SGLT2) inhibitor is a new antidiabetic drug, included in the family of sodium-glucose transporters. It controls hyperglycemia, hypertension and hyperlipidemia; therefore it is mainly dedicated to diabetic patients at risk of developing chronic heart failure. Recent studies have revealed that SGLT2 is found not only in the proximal convoluted tubules S1 and S2 in kidneys but also in the lens and the retina [51].
SGLT2 plays the role of a retinal glucose sensor; Na+-dependent glucose cellular concentration causes pericytes swelling, destruction and increased retinal vascular leakage [52]. By preventing pericyte swelling SGLT2 inhibitor postpones vascular changes and could be a successful treatment choice in an early stage of DR.
Vascular diameter changes play a significant role in development and progression of DR. Multiple studies have proved that wall to lumen ratio (WLR) and cross-sectional area of arteriolar wall growth correlate with the onset and the severity of DR [53]. Green et al. studied dapagliflozin influence on the retinal microvasculature and found no increase in the retinal wall-cavity ratio after the treatment [54]. Moreover, the study emphasized dapagliflozin’s role in the retinal capillary flow decrease and vascular hyperemia prevention.
Several studies revealed a possible connection between SGLT2 expression and the sympathetic nervous system (SNS), as early autonomic disorders have been found in DR patients. SNS activation, which is indicated by norepinephrine occurrence, increases kidneys’ SGLT2 expression and correlates with nerve damage in the outer layer of the retina [54]. However, these interactions should be investigated thoroughly in further clinical studies.
Although SGLT2 has wide therapeutic potential in general diabetic treatment, its efficacy as a DR drug has been evaluated only in animal model-based studies and should be examined in future research.
Islet cell transplantation
Islet cell transplantation (ICT) has been commonly used in diabetes treatment since the early 1990s. Extensive research has tried to examine the effectiveness of pancreas transplantation in DR therapy, supporting the stability of retinal changes after the procedure [55]. Thompson et al. conducted a prospective, crossover, cohort study comparing medical treatment and islet cell transplantation efficacy in DR progression prevention in a 3-year follow-up. The 44 patients were 20 to 65 years of age, with a history of more than 5 years of diabetes duration; they underwent multiple eye fundus examination with possible macular edema evaluation [56]. Progression was defined as a need for laser treatment or one step worsening along the international disease severity scale [56].
The results revealed significant discrepancies in both groups. Posttransplant patients had better hyperglycemia control and progression was observed more often in the medical group than in ICT subjects (12.2% vs. 0%) [56]. Possibly the better effect of IST may be due to the increase of retinal blood flow after the therapy [57]. There was a significant difference between the two groups in post-ICT immunosuppression, which did not have any previously documented effect on DR progression.
Although Thompson et al. found that DR progression is less probable in post-ICT patients than after intensive medical therapy usage, their study was not randomized and the determination of endpoints was not masked, which should be changed in the future.
Conclusions
Traditional therapies including drugs controlling hyperglycemia, laser therapy, vitrectomy, and intravitreal injections of anti-VEGF are widely applied in DR patients with satisfactory therapeutic effects. Although these treatments are effective in retinal neovascularization or retinal macular edema prevention, they have some limitations in clinical application. New therapies are bringing new mechanisms such as gene control, enhancement of regenerative potential of retinal pigment epithelium focusing on the minimal possible side effects. Recent treatments were proved to be successful in pathological neovascularization prevention; however, most of the therapeutic studies remained at the basic research stage or were conducted on animal models. Hopefully, more randomized, human based studies will be carried out in the future with high-quality positive clinical therapeutic evidence.