




Papillary fibroelastoma is a benign cardiac tumor, generally small and with papillary fronds, third in frequency after cardiac myxoma and lipoma, with a prevalence of about 10% of all cardiac tumors [1, 2]. Its localization, similarly to other benign cardiac tumors, prefers the endothelium of the valve leaflets, most commonly the aortic valve (44% to 59%), less frequently the mitral (13% to 35%) and tricuspid (4% to 15%) valves [3–5]. It is discovered occasionally or following symptoms due to systemic or coronary embolization. Symptoms due to obstruction of the ventricular flow tract are rare. Surgical excision is curative and its recurrence rare if the resection of margins are disease-free.
In December 2020, a 58-year-old patient was admitted to the Coronary Intensive Care Unit of the Tor Vergata University Hospital for chest pain due to acute coronary syndrome involving the right coronary artery. Consequently, he underwent stent implantation on the posterior descending artery. Trans-thoracic echocardiogram performed during hospitalization showed a pedunculated and rounded right atrial mass in proximity of the tricuspid valve, between the septal and posterior leaflets.
The indication for surgery was given after stabilization of clinical conditions; therefore, the patient was discharged and re-hospitalized at our surgery division in March 2021.
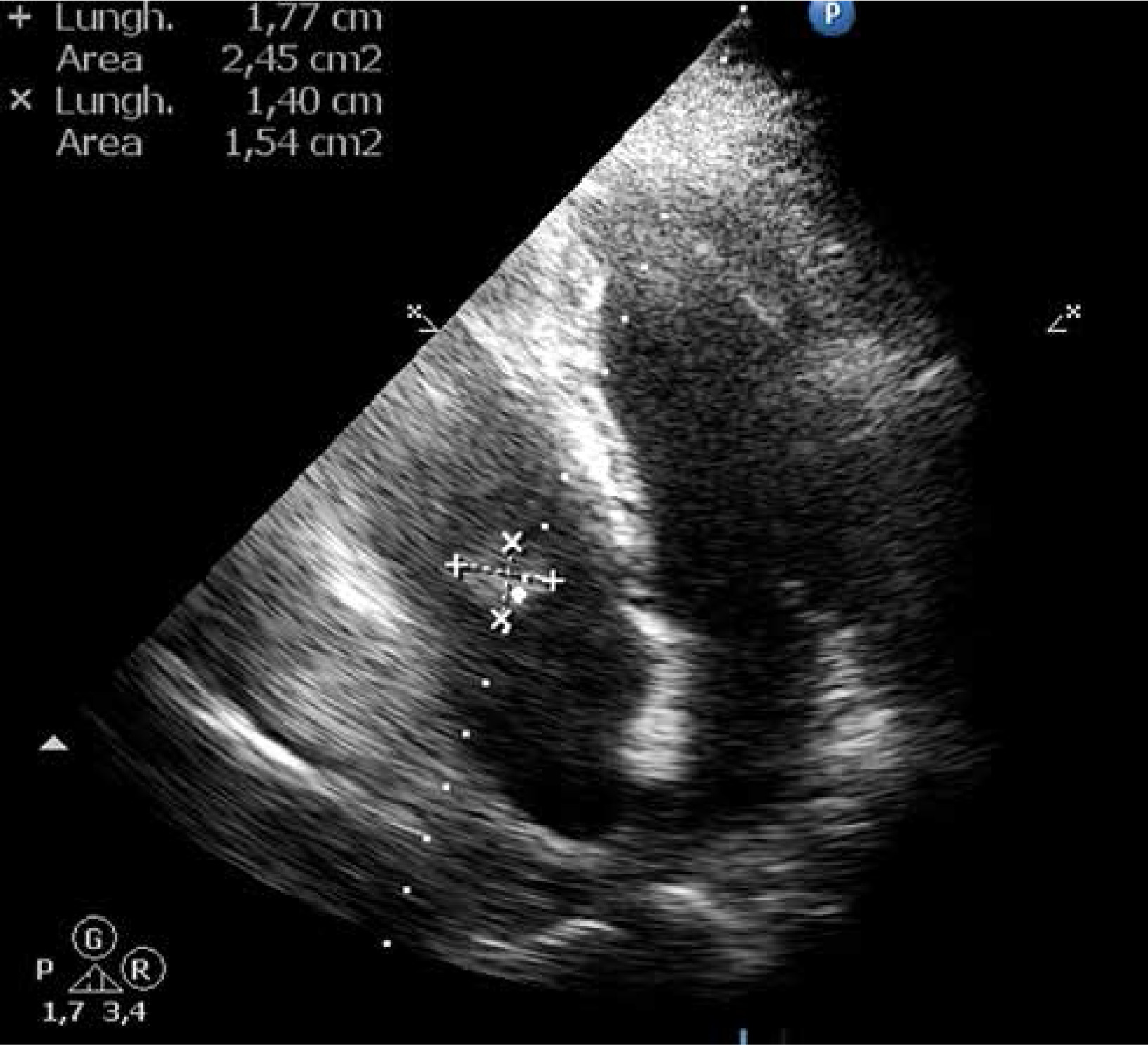
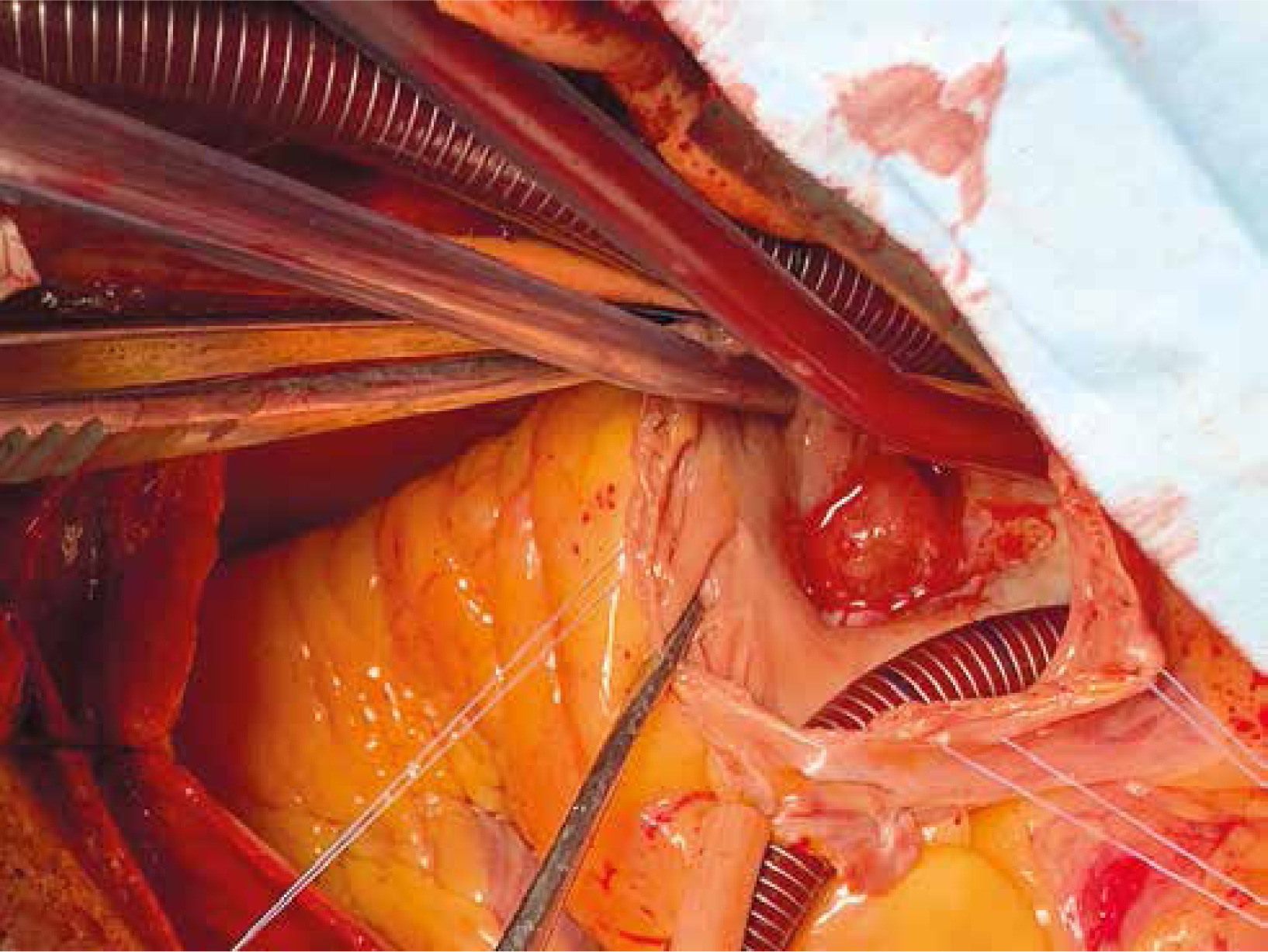
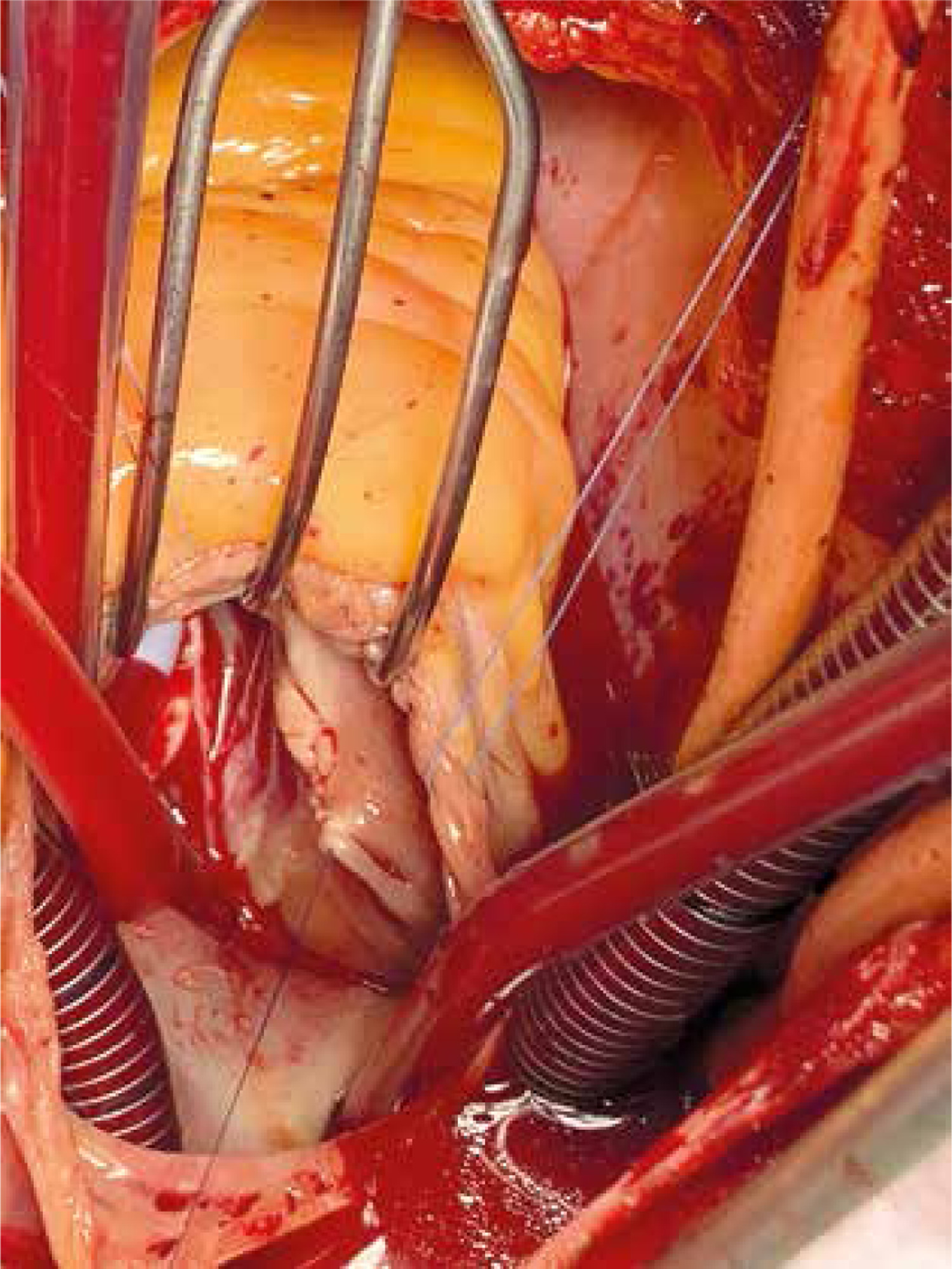
Trans-thoracic echocardiogram showed a rounded and pedunculated formation, with inhomogeneous echo structure, regular margins, with a maximum diameter of 1.7 cm × 1.4 cm, in the proximity of the free wall of the right atrium, with an implant base near the septal leaflet of the tricuspid valve, with associated moderate valve regurgitation (Figure 1). Perioperative trans-esophageal echocardiogram confirmed these findings. Following a median sternotomy, cardio-pulmonary bypass was instituted by means of aortobicaval cannulation; the heart was arrested with a single dose of cold crystalloid antegrade cardioplegia. After right atriotomy, a rounded mass, extremely mobile with a remarkably jelly-like consistency, was detected, with dimensions of about 1.5 cm × 2.0 cm, with a small peduncle of 1.0 cm in length, adhering to the septal leaflet of the tricuspid valve (Figures 2, 3). The tumor was completely removed at its base. The solution of discontinuity of the septal leaflet remained after removal of the tumor was reconstructed by means of a double continuous 5.0 polypropylene suture (Figure 4).
Figure 1
Preoperative trans-thoracic echocardiography showing a single mass in the right atrium in continuity to the tricuspid valve

The right atriotomy was closed, the aortic clamp was removed, and the patient was weaned from cardiopulmonary bypass. Trans-esophageal echocardiogram did not show residual tricuspid valve regurgitation.
Histological examination diagnosed a gelatinous-mucoid consistency mass compatible with a papillary fibroelastoma. The postoperative course was uneventful, and patient was discharged on the seventh postoperative day.
One-month follow-up echography showed no recurrence of disease and normal tricuspid valve function.